Autoantibody Detection for the Differentiation of Autoimmune Liver Diseases

Complete the form below to unlock access to ALL audio articles.
Autoimmune liver diseases (ALDs) are characterized by the production of autoantibodies against cells of the liver and biliary system. There are three main ALDs: autoimmune hepatitis (AIH), primary biliary cholangitis (PBC) and primary sclerosing cholangitis (PSC). Symptoms of ALD vary among patients and can include non-specific symptoms such as fatigue, pruritis and nausea.1 Early treatment of ALD can prevent liver damage and the need for liver transplant. Therefore, prompt diagnosis is imperative for patients with ALD. Because treatments differ for ALDs, it is necessary to differentiate between the three diseases. In cases of suspected ALD, testing for liver-related autoantibodies should be performed (Table 1).
Autoimmune Hepatitis (AIH)
AIH is the most common ALD, with a prevalence of 4 to 42.9 per 100,000 persons depending on geographic region.2 While the etiology of AIH is unknown, AIH leads to destruction of hepatocytes and can result in cirrhosis and end-stage liver failure, with a high mortality rate if left untreated.3
Guidelines from the American Association for the Study of Liver Diseases (AASLD) require histological findings compatible with AIH, such as interface hepatitis, to make a diagnosis.4 The diagnosis is supported by the presence of elevated serum aminotransaminase, elevated serum IgG and/or serological markers and the exclusion of other diseases that may resemble AIH. Additionally, autoantibodies are a hallmark of AIH detected in more than 80% of patients.5-7
The identity of autoantibodies present classifies patients as either type 1 or type 2. In the US, 96% of adults with AIH have type 1,8 but type 2 is more prevalent in children.9 Type 1 is classified based on the presence of antinuclear antibodies (ANAs) and/or anti-smooth muscle antibodies (ASMAs). Filamentous (F)-actin antibodies, a subset of ASMAs, are found in 86–100% of AIH patients with ASMAs.10 Antibodies to soluble liver antigen/liver-pancreas antigen (SLA/LP) are the most specific markers of AIH (99% specificity),11 and are also associated with severe disease and risk of relapse during treatment.12
Type 2 AIH is characterized by anti-liver/kidney microsomal antibody type 1 (LKM-1), often in the absence of ANAs and ASMAs.3 Additionally, antibodies against LKM-3 and/or liver cytosol type 1 antigen (LC-1) are infrequently detected.4
According to AASLD guidelines, ANAs and ASMAs should be tested for if AIH is suspected in adult patients, followed by LKM-1 testing if the patient is ANA- and AMA-negative. However, ANAs, ASMAs and LKM-1 antibodies should all be assessed during initial testing in pediatric patients. In the absence of these autoantibodies, further serological testing may include detection of anti-SLA/LP, as well as autoantibodies that may help rule out diseases such as PBC, PSC or celiac disease.3
According to the International Autoimmune Hepatitis group, indirect immunofluorescence assays (IFAs) on a combination of rodent kidney, liver and stomach tissue is the preferred screening technique for detection of AIH-relevant antibodies.11,13 This combination of substrates enables detection of ANA, ASMA, anti-LKM-1 and anti-LC-1. However, anti-LC-1 can be masked by anti-LKM staining on rodent liver; therefore, solid phase assays are useful to detect anti-LC-1.14 Upon ANA positivity on rodent tissue, ANA patterns should be assessed using HEp-2 cells.11
Based on IFA patterns, monospecific assays such as ChLIA, ELISA or immunoblot should be used as confirmation.13 Additionally, F-actin can be also confirmed through IFA on fibroblasts or vascular smooth muscle cells (VSM47).15 Notably, anti-SLA/LP must be tested with ChLIA, ELISA or immunoblot because these antibodies cannot be detected with tissue-based IFA.13
Primary Biliary Cholangitis (PBC)
PBC is an autoimmune liver disease that is characterized by chronic non-suppurative granulomatous inflammation of the small intrahepatic bile ducts.16 The disease can ultimately result in end-stage biliary cirrhosis and liver failure if left untreated.16 Importantly, patients respond best to treatment earlier in the disease, emphasizing the need for prompt diagnosis.17
The diagnosis of PBC mainly relies on the detection of autoantibodies, especially anti-mitochondrial antibodies (AMAs), which are found in 95% of patients with PBC.17,18 According to AASLD guidelines, patients with evidence of cholestasis based on elevated alkaline phosphatase (ALP) levels and serum AMAs or other PBC-specific autoantibodies do not require a biopsy for diagnosis.16 Additionally, the presence of AMAs can predict the development of PBC in asymptomatic patients without abnormal liver function tests.19 Anti-M2 AMAs mainly target the E2 subunits of the pyruvate dehydrogenase complex (PDC), the branched-chain oxo glutaric acid dehydrogenase complex (BCOADC) and the oxoglutarate dehydrogenase complex (OGDC). To a lesser extent, Anti-M2 AMAs also recognize the E1 and E3 subunits.20
If PBC is suspected in the absence of AMAs, the patient should be tested for ANAs.13 Antibodies to Sp100 and PML are fairly specific for PBC and result in a “nuclear dots” pattern on HEp-2 cells.21-23 Additionally, some patients may exhibit anti-gp210 or anti-lamin-B-receptor antibodies, which result in a “nuclear membrane” pattern on HEp-2 cells and are specific for PBC.24,25 Rarely, anti-centromere antibodies are also observed in PBC patients but are not specific to the disease.13
As in AIH, IFA on rodent tissue should be performed as initial screening for PBC. IFA on rat kidney is the gold standard for detection of AMAs.26 Following positive IFA results, monospecific tests such as ELISA or immunoblot should be performed as confirmation.16,27 A previous study found that an ELISA using native PDC and a recombinant peptide consisting of the E2 subunits of BCOADC, PDC and OGDH as the antigen substrate shows increased sensitivity compared to the conventional M2 ELISA, allowing the detection of AMAs in 30–50% of previously negative samples.20
Primary Sclerosing Cholangitis (PSC)
PSC is a rare chronic cholestatic liver disease that is characterized by inflammation of the bile ducts, ultimately leading to cholestatic liver damage, cirrhosis and liver failure.28 Notably, 50–80% of patients with PSC also have a chronic inflammatory bowel disease (CIBD), most frequently ulcerative colitis (UC).29 Therefore, ALD should be considered during the work-up of abnormal liver function tests in patients with CIBD.
The diagnosis of PSC is mainly based on magnetic resonance cholangiography, although liver biopsy can assist in diagnosing patients with a normal cholangiogram.30 While serum autoantibodies can be observed in PSC, they are highly variable between patients and provide limited diagnostic utility.13 The most common autoantibodies observed in PSC are antineutrophil cytoplasmic antibodies (ANCAs), ANAs and ASMAs, but these antibodies are not specific for PSC.31 ANCAs are also common in UC patients without PSC;32,33 therefore, ANCAs are useful to support a diagnosis of PSC only in patients without a concomitant CIBD.
Conclusions
The detection of autoantibodies is indispensable for a rapid and accurate diagnosis of ALD and can also prevent the need for invasive liver biopsies. ALDs share non-specific symptoms; therefore, diagnosis cannot be based on clinical presentation alone. While autoantibodies have minimal diagnostic use for PSC, autoantibodies are hallmarks of AIH and PBC and are required for diagnosis.
While some labs rely on monospecific tests for ALD screening, IFA screens on a combination of rodent liver, kidney and stomach allow for the simultaneous detection of most ALD-associated autoantibodies.13 When ChLIA, ELISA or immunoblots are used for screening, positive patients may be missed if the relevant autoantigens are not included in the assay.
Recent studies have identified additional autoantibodies that may aid in diagnosis of ALD (Table 2). For example, previous work has found that D-3-phosphoglycerate dehydrogenase (3-PHGDH) antibodies are specific for AIH and that antibody titers decrease during corticosteroid treatment.34 Novel antibodies may be particularly useful to support PBC diagnosis in AMA-negative patients.35,36 Antibodies against kelch-like protein 12 (KLHL12) and hexokinase 1 (HK-1) have specificities exceeding 95% for PBC, and their combination yields a sensitivity of 75% in AMA-negative patients.36 Future studies are required to identify autoantibodies that are associated with disease course, response to treatment and disease pathogenesis.
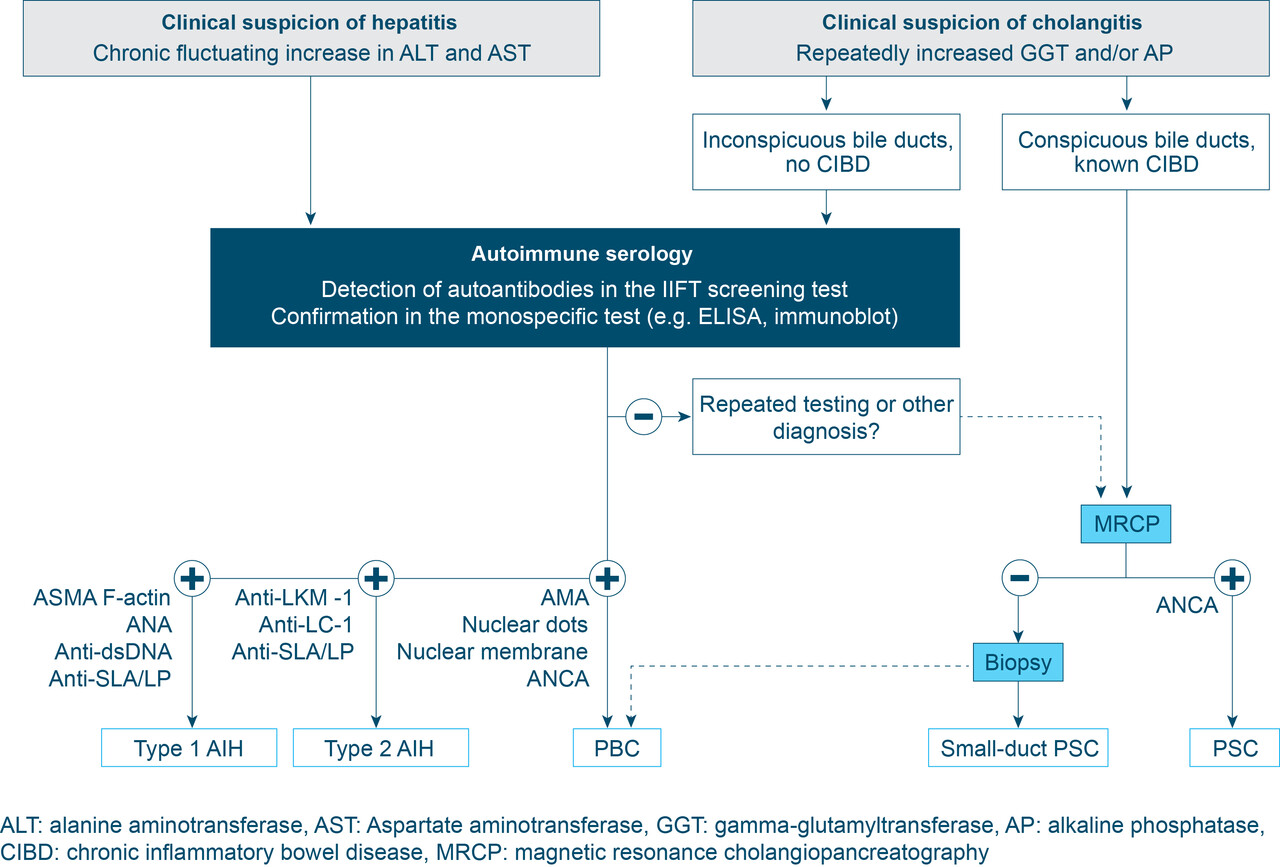
Figure 1: Diagnostic algorithm for ALD
| Disease | Autoantibody | Prevalence |
| AIH – Type 1 | ANA | 50–75%37 |
| ASMA | 63%8 | |
| Anti-SLA/LP | 7–22%38 | |
| AIH – Type 2 | Anti-LKM1 | |
| Anti-LKM3 | 17% of AIH-240 | |
| Anti-LC-1 | 30% of AIH-213 | |
| PBC | AMA | 95%18 |
| ANA | 30–50% of AMA negative patients41 | |
| PSC | Atypical ANCA | 50–88%42 |
| ANA | 8–77%31 | |
| ASMA | 0–83%31 |
Table 2: Novel autoantibodies in ALD
| Disease | Autoantibody | Prevalence |
| AIH | D-3-phosphoglycerate dehydrogenase (PGDH) | 80% untreated34 |
| Programmed cell death-1 (PD-1) | 63% of AIH-143 | |
| Asialoglycoprotein receptor (ASGPR) | ||
| PBC | Kelch-like 12 (KLHL12) | 36%46 |
| Hexokinase 1 (HK-1) | 45%36 | |
| PSC | Integrin avb6 | 89.1%47 |
| Sulphite oxidase (SO) | 43%48 |
About the author:
Jackie Weiss, PhD is the Scientific Affairs Liaison at EUROIMMUN US. Her role includes working with key opinion leaders on scientific collaborations, scientific writing, and supporting the team with commercial activities.